Ultrasound
Findings in Appendicitis
Case 1
| Non-perforated appendicitis. 14
year old male presented to the emergency department with
right lower quadrant pain. for six hours duration. On
physical examination he was febrile. Complete blood count
revealed leukocytosis. A right lower quadrant ultrasound,
shown below, was requested to evaluate for appendicitis.
|
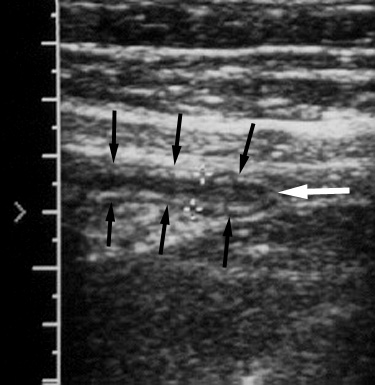 |
Longitudinal graded compression ultrasound image
demonstrates a mildly dilated appendix (black arrows)
with preservation of the expected multilayered appearance
of bowel. Note blind end of the appendix (white arrow).
There is no evidence of an appendicolith or adjacent
fluid. |
| At surgery, early non-perforated appendicitis was
confirmed. |
Return to Ultrasound
Findings
Case
2
| Perforated appendicitis. 2 year
old girl was transferred from an outside hospital with a
two day history of bilious vomiting, excessive crying,
irritability, and right lower quadrant tenderness. She
had no bowel movements during the prior two days.
Physical examination revealed a soft, non-distended
abdomen with right lower quadrant tenderness. The patient
was most comfortable with her hips flexed. An ultrasound
examination was performed to evaluate for appendicitis,
shown below.
|
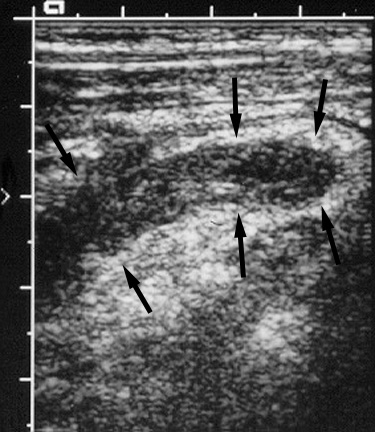 |
Graded compression ultrasound of the right lower
quadrant reveals a non-compressible, enlarged appendix
(arrows). Definition of the bowel wall layers,
particularly the echogenic submucosa, is lost, suggesting
perforation. |
| At surgery, a perforated appendix was found, without
adjacent abscess or purulent fluid. |
Return to Ultrasound Findings
Case 3
| Perforated appendicitis with free fluid. 5
year old girl with a two day history of nausea, vomiting,
fever, and abdominal pain presented to the emergency
room. An ultrasound examination was requested to
differentiate between appendicitis and ovarian torsion,
shown below.
|
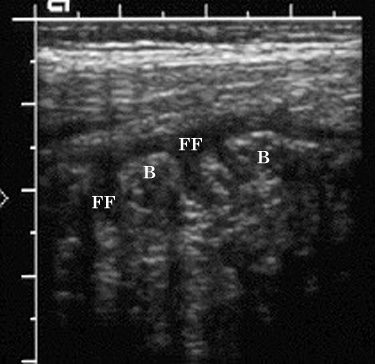 |
Figure 1. Ultrasound image of the right lower
quadrant in transverse plane shows free intraperitoneal
fluid (FF) surrounding loops of bowel (B). |
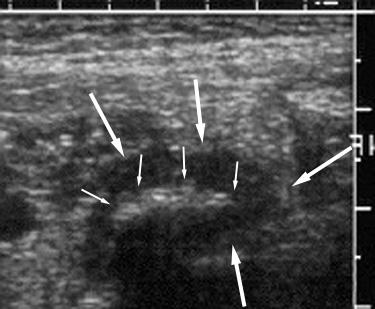 |
Figure 2. Graded compression ultrasound image lower
in the right pelvis in transverse plane, demonstrates a
calcified appendicolith (small arrows) within the dilated
appendix (large arrows).. |
| At surgery a perforated appendix with adjacent
purulent material was removed. Surgical drains were
placed in the pelvis and right paracolic gutter. |
Return to Ultrasound Findings
Case 4
| Perforated appendicitis. 10 year
old girl with a three day history of right lower quadrant
pain, intermittent nausea, vomiting, fever, and chills
presented to the emergency room. Physical examination was
significant for abdominal guarding and rebound tenderness
in the right lower quadrant. Laboratory evaluation
revealed leukocytosis. A graded compression ultrasound
examination was performed to evaluate for appendicitis,
shown below.
|
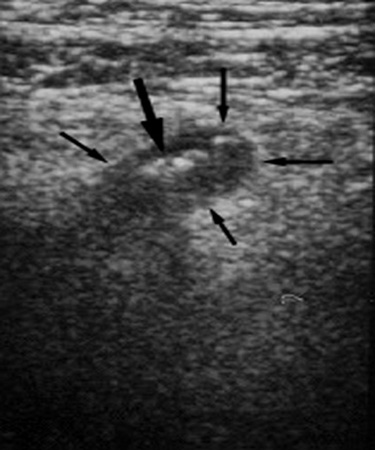 |
Figure 1. Graded compression ultrasound image of the
right lower quadrant in longitudinal plane, shows an
enlarged, non-compressible appendix (small arrows), which
contains appendicoliths (large arrow). Note that the
walls of the appendix are asymmetric, thicker posteriorly
than anteriorly, and there is loss of the expected
multilayered appearance. These findings may be associated
with perforated appendicitis. |
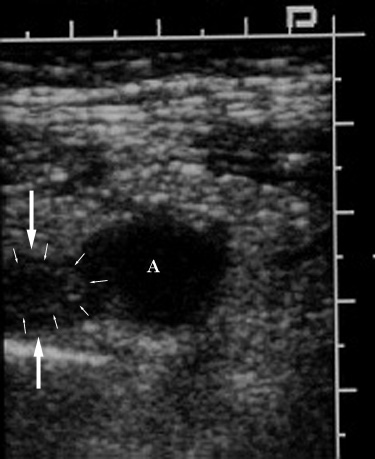 |
Figure 2. Ultrasound image obtained near Figure 1 in
an oblique plane shows an echovoid fluid collection (A)
representing a small abscess adjacent to a portion of the
abnormal appendix (large arrows). As noted above, there
is loss of the expected multilayered appearance of the
appendix; only a single echogenic layer representing the
submucosa (small arrows) is present in its tip. |
| The diagnosis of perforated appendicitis was made and
the patient was treated with intravenous antibiotics for
seven days. However fever and abdominal pain persisted,
and a CT examination was performed, shown in the CT
Findings in Appendicitis section. |
Related teaching points can also be found in Primary Treatment
Return to Ultrasound Findings
Case 5
| Perforated appendicitis with multiple
appendicoliths and ileus. 1 year old girl
presented to the emergency room with one day history of
abdominal distention and fever. A plain abdominal
radiograph was obtained which revealed several calcified
appendicoliths in the right lower quadrant, as well as
several dilated small bowel loops (refer to Plain Film Findings for
additional details). An ultrasound was subsequently
performed to evaluate for appendicitis, shown below.
|
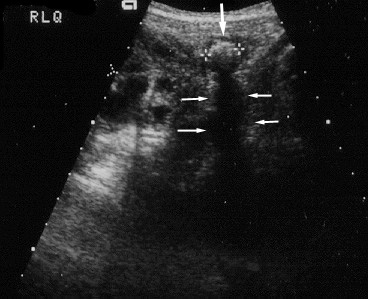 |
Figure 1. Graded compression ultrasound of the right
lower quadrant in transverse plane, reveals a calcified
appendicolith (arrow) within the dilated appendix
(electronic cursors). Note the well-defined posterior
acoustic shadow (small arrows) in relation to the
appendicolith. |
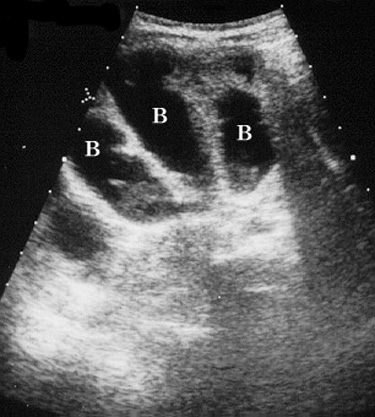 |
Figure 2. Transverse ultrasound image of the mid-
abdomen demonstrates multiple dilated, fluid-filled bowel
loops (B) consistent with an ileus. Small bowel
obstruction could produce similar findings. |
| At surgery, an inflamed, perforated appendix was
removed |
Return to Atypical
Clinical Presentation (C)
Return to Ultrasound Findings
Case 6
| Perforated appendicitis associated with
shigellosis. 5 year old boy status post
meningomyelocele repair and ventriculoperitoneal shunt
placement presented to the emergency room with abdominal
pain and diarrhea for one day. He was diagnosed and
treated for shigellosis. However, abdominal pain
persisted, and peritoneal signs developed. Ultrasound
examination (shown below) was requested to exclude an
abscess.
|
 |
Figure 1. Longitudinal pelvic sonogram
through the right lower quadrant shows a
multiloculated fluid collection (FC). One of the
loculations contains debris (D) of low-level
echogenicity. |
|
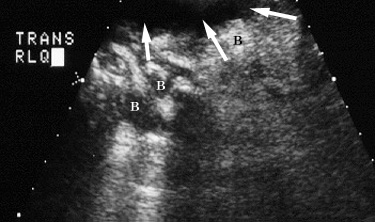 |
Figure 2. Transverse sonogram of the right lower
quadrant shows free fluid (arrows) adjacent to bowel
loops (B) |
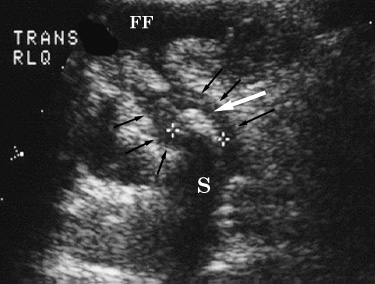 |
Figure 3. Transverse pelvic US image at a lower level
than Figure 2 shows an appendicolith (large white arrow)
within the dilated appendix (small black arrows). Free
fluid (FF) is noted anteriorly. Note posterior acoustic
shadow (S) related to the appendicolith. |
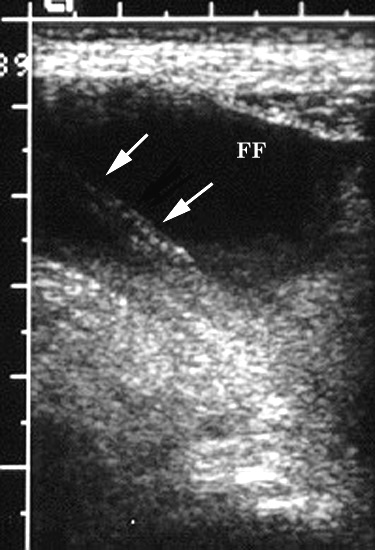 |
Figure 4. Longitudinal US image of the mid-lower
abdomen demonstrates the ventriculoperitoneal shunt tube
(arrows) within free intraperitoneal fluid (FF). |
| At surgery a perforated inflamed appendix with pus in
the peritoneal cavity was found. Patient underwent
appendectomy and externalization of the
ventriculoperitoneal shunt. |
Return to Ultrasound Findings
Case 7
| Appendicitis mimicking pelvic inflammatory
disease. 18 year old nonpregnant sexually
active female who presented to the emergency department
with right lower quadrant pain. On pelvic examination,
she had cervical motion tenderness. Pelvic ultrasound,
shown below, was requested to evaluate for pelvic
inflammatory disease. Graded-compression right lower
quadrant ultrasound, not shown, did not identify the
appendix .
|
 |
Figure 1. Transverse endovaginal ultrasound image
shows a complex cystic right adnexal mass (arrows)
thought to represent a tubo-ovarian abscess. The right
ovary was not seen. U = uterus. |
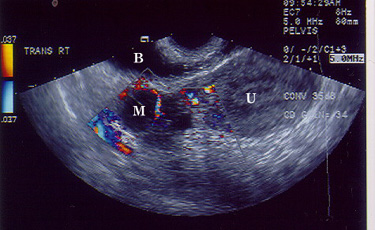 |
Figure 2. Transverse endovaginal color Doppler
ultrasound image shows increased vascularity to the solid
components of the right adnexal mass (M). U = uterus. B =
urinary bladder. |
| The patient was taken to surgery because of clinical
deterioration. Perforated appendicitis with abscess
extending into the right pelvis was identified. |
Return to Ultrasound Findings