Appendicitis

Describe the pathological changes of acute appendicitis.
- Appendix is inflamed.
- The lumen is filled with neutrophils.
- The mucosa is ulcerated.
- There is inflammation of visceral and parietal peritoneum.
- Appendiceal inflammation is associated with obstruction in 50 to 80% of cases (due to fecalith, tumor or ball of worms - oxyuriasis vermicularis).
What are the imaging procedures useful in the evaluation of a patient suspected to have appendicitis?
- CT scan
- Ultrasound
- Plain abdominal radiograph
What are the potential complications of acute appendicitis?
- Perforation (most serious)
- Pylephlebitis with thrombosis of the portal vein
- Liver abscess
Discuss the utility of each imaging procedure.
- Role of CT:
- CT scan is the most ideal imaging procedure for diagnosing appendicitis and its complications.
- Spiral CT is useful when you are not quite sure of the diagnosis from the history and physical exam and there may me cofounding variables such as old age and/or other morbidities.
- Appendiceal CT showed the highest sensitivity and specificity, among the radiologic options.
- It not only enables the examiner to differentiate diffuse periappendiceal inflammation from an abscess but also detects many of the diseases included in the differential diagnosis of acute appendicitis.
- Role of ultrasound:
- Abdominopelvic ultrasound can be limited by gas in bowel.
- Ultrasound is useful in pregnant woman with abdominal pain or young children where there is clinical doubt.
- Ultrasound is reliable and sensitive for the detection of appendicoliths and the demonstration of an abnormally distended or thick-walled appendix.
- Role of plain film:
- Sensitivity for diagnosis of appendicitis is low.
- Conventional abdominal radiography along with contrast-enema radiography no longer has a role.
Is imaging procedure required in all suspected cases of appendicitis? What are the limitations with imaging procedures and the diagnosis of Appendicitis?
- When surgeon is confident of the diagnosis, he or she may opt to take the patient to OR without the need for imaging procedures.
- Despite the number of algorithms and diagnostic tests available, 20% of patients with appendicitis are misdiagnosed.
- Also, 15 to 40% of all operations performed for suspected appendicitis turn out to have normal appendices.
What is the sensitivity and specificity of each imaging procedure in diagnosing appendicitis?
- CT:
- Spiral CT has a sensitivity of 90-100%, a specificity of 91-99%, a positive predictive value of 95-97%, and an accuracy of 94-100%.
- Spiral CT has a sensitivity of 90-100%, a specificity of 91-99%, a positive predictive value of 95-97%, and an accuracy of 94-100%.
- Ultrasound:
- The limitation to ultrasound is that the appendix is often unseen due to associated bowel gas.
- When carefully performed it has a sensitivity of 75-90 percent, a specificity of 86-100 percent, and a positive predictive value of 89- 93 percent for the diagnosis of appendicitis.
- It is operator dependent
Image Atlas of Appendicitis
What are the radiological findings of appendicitis in plain abdominal radiograph?
There are no specific signs of appendicitis in plain films but you may see:
- ileus
- appendicoliths
- sentinel loop (dilated adjacent ileum)
- evidence for complications like perforation or appendiceal abscess
- widening and blurring of peritoneal fat line
- right lower quadrant haze due to fluid, edema and mass
- mass indenting the cecum
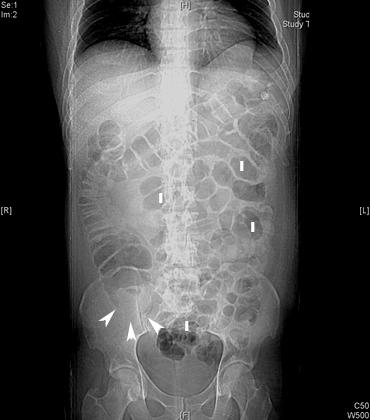
Acute Appendicitis
-
Arrowheads point to a soft-tissue mass producing deformity of the cecal air.
-
I: Ileus

Appendicolith
Findings:
- Plain film showing appendicolith.
- Arrow points to ileus.
- Appendicolith may be seen without clinical signs of appendicitis.
What are the radiological findings of appendicitis in abdomen CT?
- Ileus: Dilated loops of bowel
- Appendix > 6mm in diameter
- An appendicolith
- Failure of the appendix to fill with oral contrast medium
- Enhancement of its wall with intravenous contrast medium
- Periappendiceal inflammation/inflammatory infiltration of fat
- Free fluid in cul de sac
- Abscess
- Inflammatory (phlegmon) mass
- Air pockets
- Contrast enhancement
- Extraluminal gas from perforation
- Pericecal lymphadenopathy
- Cecal wall thickening
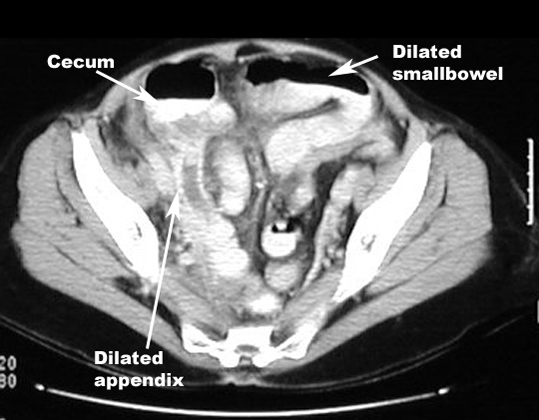
-
Dilated appendix
-
Dilated loops of bowel
Acute Appendicitis

Appendicolith
- Arrow points to the appendicolith. Arrowhead points to the appendix.
- Arrow points to the thickened bowel wall. Arrowheads point to inflammatory infiltration of the fat.
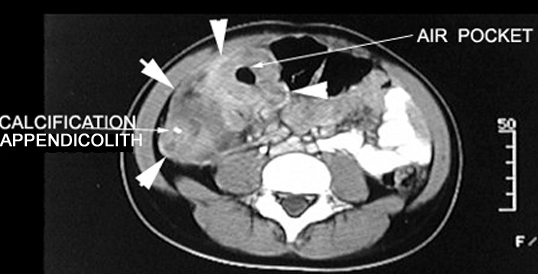
Acute Appendicitis Appendiceal abscess
Arrows point to the inflammatory mass in the right lower quadrant with an air pocket, indicating an abscess.
Mass demonstrates contrast enhancement.
What are the radiological findings of appendicitis in abdomen ultrasound?
- The most sensitive sign of appendicitis from ultrasound is a non compressible appendix with a diameter of 7mm or greater.
- Other findings may include:
- appendicolith
- thickened appendiceal wall
- abscess
- fluid around the appendix
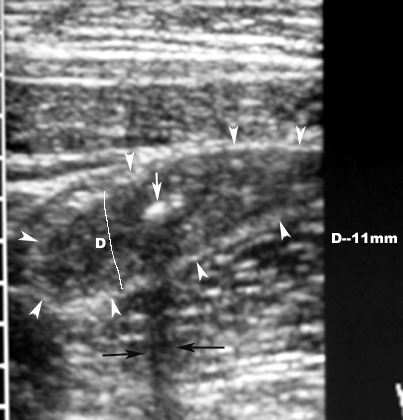
Appendicitis with Appendicolith
Findings:
- White arrow points to appendicolith.
- D is the diameter of the appendix measuring more than 7 mm.
- Arrowheads point to distended appendix.
- Black arrows point to posterior shadowing.