Describe the characteristic pathologic changes
- The lung shows acute inflammation.
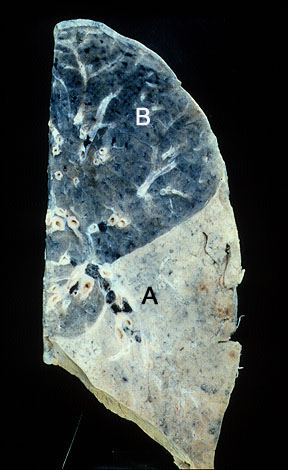
- Lobe is consolidated
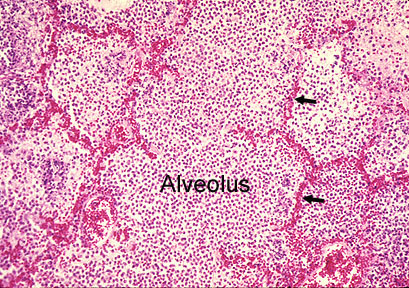
- Alveoli are filled with fibrin and inflammatory cells, predominantly neutrophils.
- Interstitial capillaries are congested.
- Bronchioles are filled with inflammatory cells.
- The pleura is edematous and contains some inflammatory cells.
Gray hepatization stops abruptly at the fissure.
Anticipated findings in CXR in a patient with pneumococcal pneumonia
1. Lobar density (RUL Consolidation)
- Lobar consolidation is characteristic for pneumococcal, mycoplasma and legionella pneumonia. There are many other patterns of pneumonia based on the etiological agent, ranging from broncho-pneumonia, necrotizing pneumonia, diffuse aleveolar pneumonia, interstitial pneumonia etc.

This low power photomicrograph shows many alveolar spaces filled with inflammatory infiltrate. The high power photomicrograph showed the infiltrate to be composed of neutrophiles. Note that the alveolar septa are relatively normal. After complete resolution, the underlying lung architecture is preserved.
2. No significant loss of lung volume (White arrows pointing to transverse fissure)
- Alveoli are filled with inflammatory exudate, hence the volume of lung expands slightly and remains close to normal size even at the stage of resolution.
3. Air bronchogram
(Black arrowheads pointing to air bronchogram)
- Bronchi beyond 3-4 order of branching is not recognizable in CXR, because of loss of thickness and no contrast between intra bronchial air and surrounding alveoli containing air.
- In pneumonia the disease is primarily in the alveoli. Bronchi are patent. Air in the alveoli is replaced by inflammatory exudate. Now bronchi containing air is visible because of the contrast provided by liquid density induced by inflammatory exudate
