|
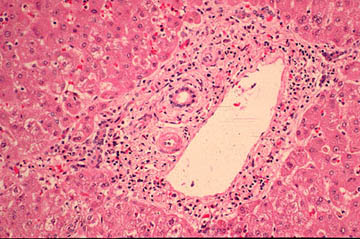
-Rounding an edema of the portal tracts. Inflammatory reaction with lymphcyte, histiocytes an some neutrophils especially in and around portal bile ducts.
|
li-11-10
INFECTIOUS CHOLANGITIS By. Dr. E OrfeiDefinition
A septic clinical condition due to infection or infestation of the biliary tract.
Etiology
The organisms causing infection a most commonly the enteric aerobic from the small intestine: E. Coli, Klebsiella. Streptococcus faecalis, Pseudomonas aeruginosa.
Pseudomonas invasion of the biliary tract is greatly favored by surgical procedures.
Among the anaerobes, Bacterioides and Clostridia are present in patients who had repeated biliary operations especially bile duct/intestinal anastomoses.
Infections of the biliary tree by protozoa, fungi (candida) and viruses (CytoMegaloVirus)
are rare. Cryptosporidia showed their increasing presence in cases of AIDS.
Pathogenesis
The most evident source of infection is the duodenum. While in normal conditions the duodenum and jejunum contain only rare Gram positive bacteria, in cases of reduced blood flow due to any type of biliary obstruction, they contain rich colonies of bacteria which invade the biliary tree. The most favoring condition for this invasion is cholelithiasis because it produces intermittent obstruction which does not occur in obstruction caused by a firm constricting tumor.
The other possible route for microorganisms to reach the biliary tree is the portal blood.
After they have reached the liver, they are eliminated in the bile and here the will form their colonies a cause the infection.
It is obvious that any instrumental invasion of the biliary tree may introduce bacteria and cause infection.
For the establishment of a biliary infection is needed an increase of pressure in the biliary tract which, with a normal pressure (8-12 mmH2O) is safe. Regurgitation of bile into the blood stream occurs when the biliary pressure goes over 15-20mmH2O.At that point the bacteria enter the blood circulation through the intracellular and lymphatic pathways.
Clinical Features
Acute cholangitis:
-Charcot’s triad: pain, fever and jaundice. It is due to calculous obstruction and purulent infection. Sometimes only fever with pain or with jaundice. If the infection is not treated, it may cause confusion and hypotension thus developing into Reynolds pentad. Also, at this stage , renal failure may occur. Decompression of bile ducts is mandatory.
A serious complication of infectious cholangitis which carries a poor prognosis is formation of a Pyogenic liver abscess. This forms in the majority of cases after a non recognized or inadequately treated acute cholangitis. Other causes include intra-abdominal sepsis such as acute salpyngitis, perinephritis, with portal pyemia and bacterial infection of an amebic abscess.
Recurrent pyogenic cholangitis (Oriental cholangiohepatitis).
In Hong Kong and South-east Asia and , less frequent , in Columbia, Italy and South Africa, there is an acute recurrent cholangitis with bile ducts filled with bacteria like the colon together with sludge, pus and brown pigment stones. The etiology is uncertain. It is puzzle to discover how the bacteria invade the biliary tree in such number. Liver function tests demonstrate cholestasis. Ultrasound and CT scan may show intra and extrahepatic bile duct dilatation and stenoses and intaductal calculi and air. Sometimes the process may involve disproportionately only one lobe of the liver.
Pathology
|
-Rounding an edema of the portal tracts. Inflammatory reaction with lymphcyte, histiocytes an some neutrophils especially in and around portal bile ducts.
|
|
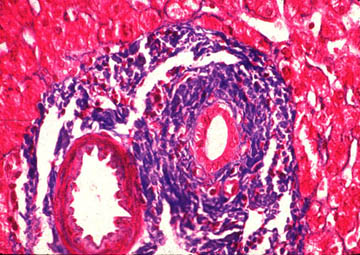
Intralobular cholestasis increases The portal bile duct is surrounded by concentric fibrosis. Medium and large ducts are most affected. Some portal fields instead of fibrosis may show inflammatory changes and loss of bile ducts. |
|
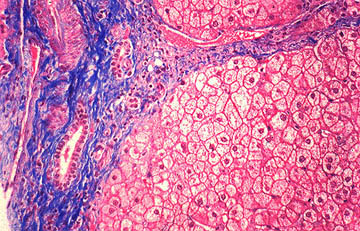
Intralobularly there may be heavy bile lakes and presence of foamy histiocytes (xanthomatous cells). Periportal fibrosis develops with proliferation of bile ductules surrounded by fibrosis at the periphery of the portal field.
|
|
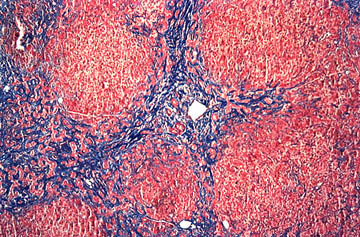
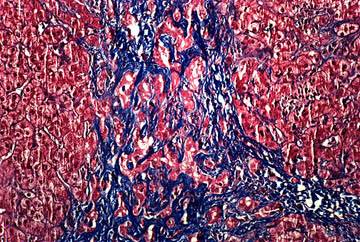
The periportal fibrosis progresses to formation of porto-portal bridges dissecting the hepatic parenchyma in nodules (dissection nodules). Hepatocytes trapped in the connective tissue septa form cholangioles. |
|
Fibrous septa with marked cholangiolar regeneration and pericholangiolar fibrosis. There is no inflammation. At this stage there is marked cholestasis.
|
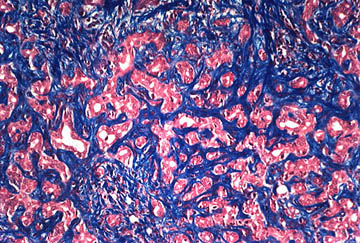 High power view of previous septum with marked cholangiolar
regeneration and fibrosis. After long time this stage may develop
cirrhosis which will be characterized by a green liver from cholestasisFig-11-10-6.Pre-cirrhotic
stage..
This type was called at one time cirrhosis of Hanot.
High power view of previous septum with marked cholangiolar
regeneration and fibrosis. After long time this stage may develop
cirrhosis which will be characterized by a green liver from cholestasisFig-11-10-6.Pre-cirrhotic
stage..
This type was called at one time cirrhosis of Hanot. |