Q1: Describe the characteristic pathologic features of heart and lungs in congestive heart failure.
- Heart is enlarged.
- Changes in cardiac chambers and myocardium depend on the etiology of heart failure.
- Irregular fibrosis replaces myocardium.
- Lung shows severe, chronic passive congestion.
- Vessels, including alveolar capillaries, are congested as a result of pulmonary venous hypertension.
- Alveoli contain numerous hemosiderin laden macrophages.

The frothy liquid oozing from the cut surface of the lung is caused by air moving through water in the respiratory tree.
Q2: Anticipated findings in chest x-ray in a patient with congestive heart failure. The following images exemplify findings of congestive heart failure in CXR.
Cardiomegaly:
- The heart is considered enlarged if the transverse diameter of the heart is larger than diameter of the hemi thorax.
- Cardiac width is larger than half trans thoracic diameter. Cardiothoracic ratio >0.5.
- You can encounter normal size heart in acute myocardial infarction or in volume overload.

Vascular phase:
- This is the first phase of congestive heart failure.
- It represents pulmonary venous hypertension.
- Cephalization: Vessels in upper chest is more prominent as a manifestation of pulmonary venous hypertension.
- Note the blood vessels are more prominent in the upper lung fields compared to the lung base, just the opposite of normal.
- In supine film the vessels are same size in upper and lower lung fields.
- You see increased (>1) artery to bronchus ratio at hilar level.

Hilar fullness with haziness:
- Enlarged pulmonary veins with perivascular fluid collection leads to full hazy hilum and vessels.

Interstitial phase:
- Kerley lines are 2-3 cm long horizontal lines in the base of lungs close to chest wall.
- They are the result of interstitial edema and increased lymphatic drainage.
- This is the second phase of congestive heart failure.

Alveolar phase:
- This x-ray shows normal size heart with bilateral diffuse soft fluffy alveolar infiltrates coalescing with each other in a butterfly distribution typical of pulmonary edema.
- The heart can be normal and develop failure, as is in this case, due to acute MI.
- Pulmonary edema is the primary manifestation of heart failure when the left ventricle acutely fails.
- In chronic heart failure is where you see vascular, interstitial, alveolar phases and pleural effusions.

Pleural effusions:
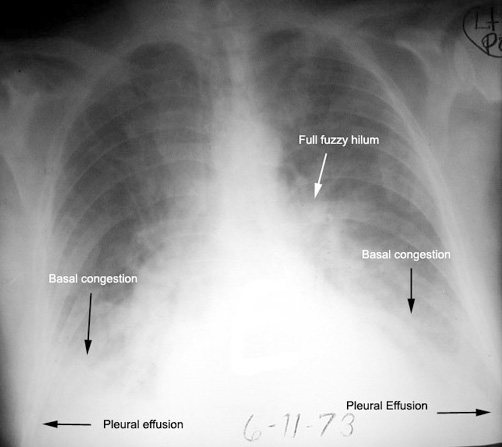
This x-ray shows:
- Cardiomegaly
- Basal congestion: This is gravity dependent accumulation of fluid in the lungs and alveoli are filled with fluid.
- Fuzzy full hilum: Represents enlarged pulmonary veins and fluid around them.
- Bilateral pleural effusions. Due to increased hydrostatic pressures.

Rapid changes in CXR: CXR can dramatically change in CHF rapidly as in this case in one day, unlike other chronic diseases.
Q4: How do you distinguish Pulmonary edema from ARDS in CXR?
- In ARDS the heart is normal in size and there are no pleural effusions.
- Clinical setting and the wedge pressure are necessary in some cases.
- ARDS is always preceded by a major event like trauma, surgery, bleeding etc. If there is no preceding major event do not consider ARDS.
Q5: What did you understand by the terms congestive heart failure and pulmonary edema?
In chronic heart failure we see lungs going through three phases: Vascular (Cephalization), Interstitial phase (Kerley lines) and alveolar phase (pulmonary congestion).
In acute left ventricular failure we see pulmonary edema. You do not see the vascular and interstitial phase.
In CHF you see basal congestion (dependent portion) while in pulmonary edema you see diffuse white out of lungs.
Chronic heart failure
- Decide whether it is PA or AP view: Many of the findings will change in AP film
- Decide on the transverse diameter of the heart
- Look for pleural effusion
- Compare the diameter of the vessels in the upper third of lungs to lower thirds
- Compare the size of the end on view of vessel to the adjacent bronchus
- Look for hilar fullness and congestion
- Look for kerley lines
- Look for basal congestion
Acute heart failure
- Heart may be of normal size
- Diffuse white out of lungs
- Butterfly pattern: Medullary or central distribution of density
- Will not see the findings noted in chronic heart failure
How to distinguish from other acute alveolar disease
- Hemorrhage: hemoptysis, sudden drop in hemoglobin
- ARDS: Prior major event (trauma, bleeding, sepsis etc), progressive hypoxia resistant to therapy requiring ventilator management
- Pneumonia: High fever , oddball infections (influenza, mycoplasma, pneumocystis etc)